In my five part series on medications I briefly discussed the importance of having a medication list. I did not properly express how important to make sure that list is reconciled with your electronic record. It is only recently that I went through a situation in which I learned this lesson the hard way. In short, my electronic record caused two family practitioners to reject me as a new patient when my Internist died suddenly in July.
Let’s face it, those of us with multiple chronic illnesses take a lot of medications. My med list fills a sheet of copy paper when printed. It is time consuming to update the list at the physician’s office so I always provided a printed list of meds to the nursing staff each visit to save time and assumed they were updating the electronic record but in reality they would get bogged down with it because the list was long and had too many meds to cross check against the electronic record. They had to go grab the next patient, take lab samples, and my list got put aside and then forgotten in the rush of the day.
I always knew what medication I was taking. My doctor knew what I was taking. So what if the nursing staff didn’t have it right in the computer system? As a retired RN, I have a working knowledge of medications and interactions. So, no big deal, right? Wrong! Two family practitioners rejected me as a patient based on my complicated inaccurate medication list after my PCP died. Had it not been for the kindness of a doctor I use to work with as a nurse, I would still be searching for primary care. I am pleased to report when I saw him as a patient for the first time last week it was equally important to his nurse to make sure my medication list was accurate and we got it fixed!
Making sure the electronic medication record is correctly reconciled to your home list is very important for reasons far greater than my snafu in finding a new PCP. The whole goal of reconciling it is to prevent medication errors one of which is FATAL drug interactions. Every physician’s office and hospital are required to accurately record your home medication list. This can be tiresome, but it is for your safety.
I saw evidence of a serious drug interactions first hand in my nursing career. My most memorable experience was a female, middle age patient who was admitted to the hospital in acute renal failure. She had no underlying kidney disease. The doctors were stumped. It was a specialist who asked, “Did you tell the nurse about ALL the medications were taking, including herbs, vitamins, and supplements?” and her response was a “No”. Her husband brought in a 13 gallon trash bag half full of herbs and vitamins she was taking regularly thinking she was doing everything she could to be healthy. Unfortunately, there were several toxic interactions between the herbs and prescription medications that were killing her kidneys requiring emergency dialysis to get the toxins out of her blood not only to safe her kidneys but her life.
In another case that could easily happen to any of us occurred when a friend of mine was experiencing some new symptoms and saw the Nurse Practitioner at the primary care physicians (PCP) office. A few sample boxes of a new medication on the market was given. When my friend developed complications and a reason could not be discovered, a specialist was sought. After a round of additional testing still there was not a reason found for the symptoms. It wasn’t until the specialist looked at the medication record scanned into the electronic record from the PCP to find the potentially fatal interaction between the newly marketed sample medication and a long term medication on my friend’s medication list. My friend had not listed the samples on the specialists new patient paperwork. The medication regimen was changed and I’m happy to say my friend is doing well.
So, what can you do to make sure the medication you take at home matches what is on file in your electronic medical record? Here are some ideas:
- Take a written list of medications to each physician’s visit. Include ALL medications including those prescribed, samples, over the counter medications (like Tylenol, antacids, and cold medicines), herbs, vitamins, supplements. Make note of any changes in your medication regimen since your last visit. When writing your medication list, be sure to write down the exact information from your prescription bottle. (For example: Ranexa 500mg. Take 1 tablet orally twice daily.)
- When the nursing staff goes over your medication list I recommend you do not give them your list until you have gone over it together. First tell her/him about any changes and be patient while each are updated in the electronic record. Then ask her to read the list on the computer screen while you check off the medication with a pen on your list.
- Ask him/her to add any medications, including over the counter medications, herbs, vitamins, and supplements that are on your list that were not read off.
- Ask him/her to delete any meds read off that are no longer on your list.
- If you have access to your electronic record through a patient portal, use it regularly to verify that the medications listed there match your actual regimen.
Because of the lack of understanding by the public about the importance of maintaining a accurate medication list, many physician offices are requiring that you bring all your prescription and non-prescription medications to each visit so they can read the bottles themselves to verify the prescription, especially when prescribed by a different practitioner. My cardiologist requires this practice.
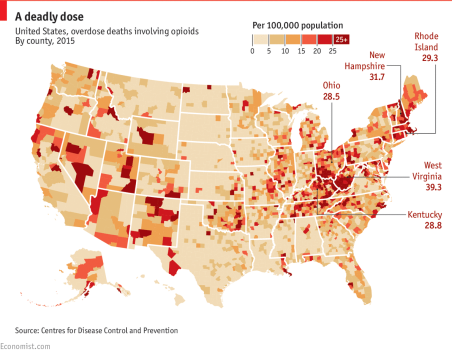
In some cases of long term prescription narcotics for chronic pain conditions, the prescribing physician is requiring the prescription bottle be presented on each visit where it is inspected for date of prescription and the remaining pills are counted and the patient is asked to give a urine sample for drug detection to verify what was prescribed shows up on the drug screen results as people are selling their narcotics on the street instead of actually taking them. The urine drug screen will also verify if the patient is taking any other narcotics.
So, drag those prescription medications, over the counter medications (including seasonal allergy medications, heartburn medications, and aspirin), vitamins, supplements, and herbs out of the bin you keep them in and put your pen to paper. Hundreds of thousands of drug interactions hospitalize Americans each year. Don’t let yourself be one of them through miscommunication about your medication regimen at home.



 As patients, we tend to forget we are paying for a service. We are consumers of healthcare services but we are treated more like the enemy than the customer. In order to advocate for patients in the past, I have likened healthcare to auto mechanic service. If you put your car in the garage and the mechanic fails to fix the car do you just say “okay”, pay him and accept your broken car? If the receptionist at the auto mechanic’s office fails to communicate that your car was ready on Friday but it’s now the following Tuesday do you say, “okay?” or do you complain about the hardship their incompetence caused you? That may seem silly but it is the same for your body which is priceless compared to a car. So, why do we accept this as the way things are in healthcare and just go on? I would suggest that we are part of the problem.
As patients, we tend to forget we are paying for a service. We are consumers of healthcare services but we are treated more like the enemy than the customer. In order to advocate for patients in the past, I have likened healthcare to auto mechanic service. If you put your car in the garage and the mechanic fails to fix the car do you just say “okay”, pay him and accept your broken car? If the receptionist at the auto mechanic’s office fails to communicate that your car was ready on Friday but it’s now the following Tuesday do you say, “okay?” or do you complain about the hardship their incompetence caused you? That may seem silly but it is the same for your body which is priceless compared to a car. So, why do we accept this as the way things are in healthcare and just go on? I would suggest that we are part of the problem.














